
















If you are planning a 10 week cycle, the goal is to be at highest blood concentrations for as many of the 10 weeks as possible.
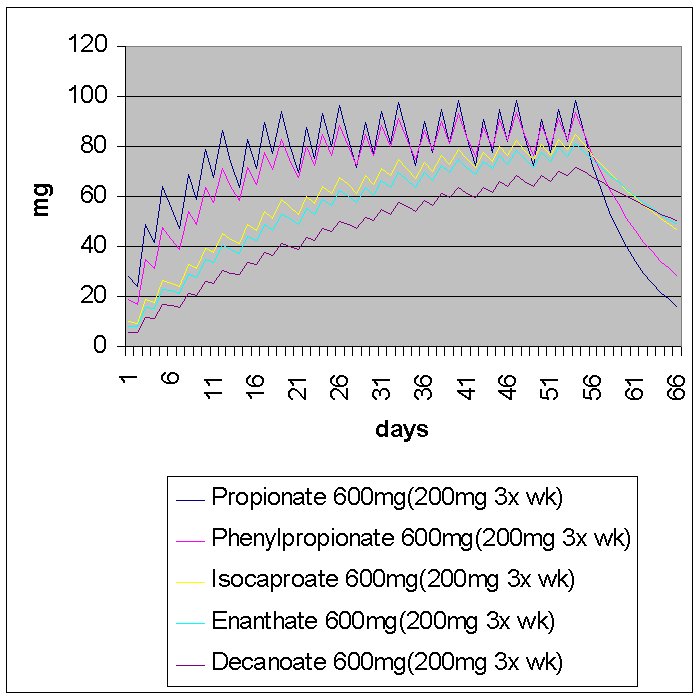
If you use a long ester such as deca at xmg/week, it will take you 4-5 weeks to build up to max blood concentrations possible for xmg/week. So half of your cycle is not wasted, but you are not maximizing efficiency.
When coming off a cycle, the waiting period before clomid therapy begins will vary depending on the type and dose of the AAS. If you ran 500mg/week of deca for 10 weeks, a month after your last shot, you will still have around 200mg of esterified deca in your system. This is more than enough to prevent recovery. This is the reason why recovery is more difficult with a deca (or another long acting ester).
Let's calculate the amount accumulated in the body after 6 weeks of 500mg/deca. Let's say you inject it once a week and we'll give it a 1.5 week half life. Note that injection frequency makes a huge difference in blood concentration stability but no difference in amount of esterified in the system
E (greek letter "sigma") 500*e^(ln(1/2)n/1.5) from n=0 to n=6. So after 6 weeks, about 1300mg of esterified nandrolone remain in the body.
Now lets see how long, after the initial injection, it takes to reduce to a small enough amount that permits recovery.
1300*e^(ln(1/2)n/1.5) After 3 weeks, 325 mg of esterified remain
after 6 weeks, 81 mg of esterified remain.
After 8 weeks, 32mg of esterified remain.
Most guys go with "time on=time off." This will not work with long esters as I have demonstrated above. For at least a month after your last shot you are in what I call a "time in-effiency" period where you are no longer reaping the benefits of you AAS but you are not recovering either. The goal of the modern cycle is to minimize this wasted time.
The key components are:
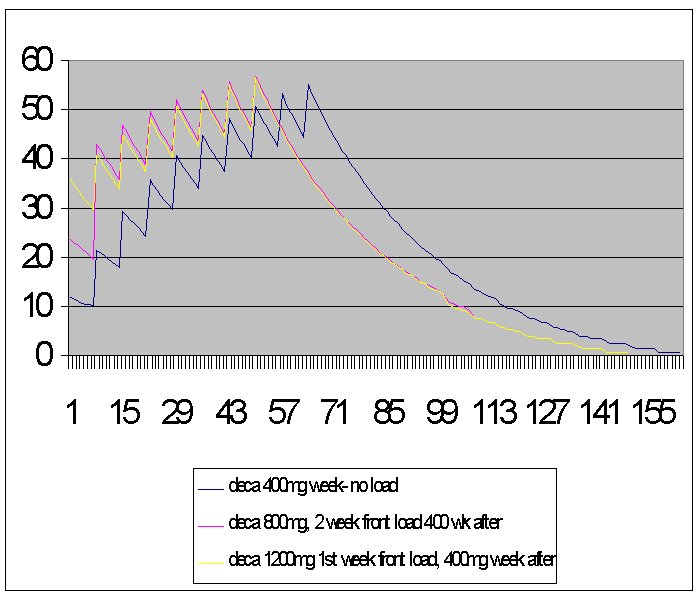
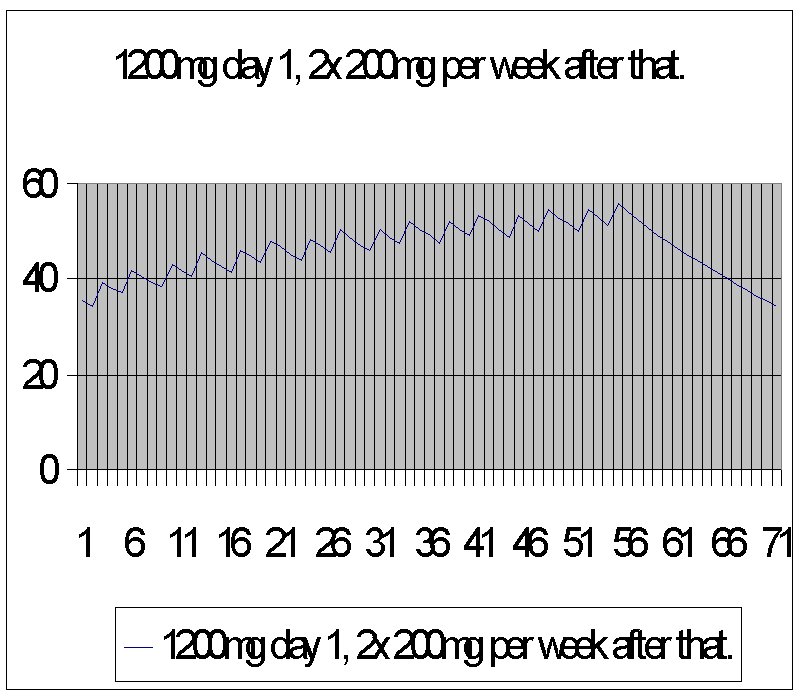
1) Front end loading this cuts down on wasted time in the beginning of your cycle waiting for the doses to reach full theraputic levels. This concept has been used before but (as far as I know) I was the first one to quantify it mathmatically. Zyg has taken the math one step further with a graph showing, visually, the importance. Graph of eq loading
The use of orals in the beginning of a cycle is a popular component of a cycle. While I don't feel it is a nessecity, it too is a (different) type of front end load. For the advnaced BBer, dbol should be taken in the beginning of a cycle as well as loading the injectables since the anabolic response from dbol is alleged to be by a different mechanism than most injectables. If one had to chose between a dbol load and and injectable load, in most cases, the injectable load should be prefered over the dbol load.
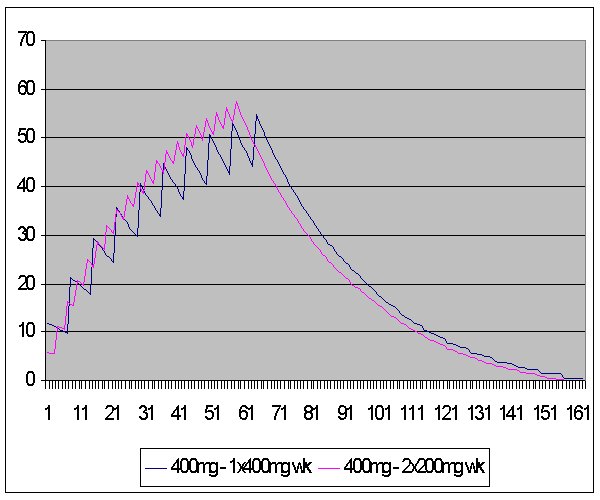
2) Injection frequency This is crucial to obtaining even blood concentrations of androgens. Ideally, the more often injected, the better. An acceptable rule of thumb is "inject at half of the half life." For instance, if the half life of a steroid is 7 days, this should be injected at least twice weekly. For cycles that involve multiple injectables, the injections should be fractioned out and divided up based on the injectable with the shortest half life. For instance, if you were doing a test propionate and deca cycle, the old school way to do it would be to inject the prop EOD and the deca once a week. Both compounds should not be viewed as separate, but together with total androgen concentration taken into consideration. If you injected the deca only once a week, probably along with one of the propionate injections, that day will have a much larger spike on total blood androgen concentrations. Instead, the deca should be split up and taken with the propionate injections, EOD. This way there is no one day of the week that has a "spike" and even blood concentrations are maintained throughout the week.
3) Ending the cycle Switching to shorter esters toward the end of a cycle makes perfect sence however not too many guys incorporate this practice- perhaps because of the lack of variety of drugs. The modern cycle should include replacing long ester injectables with shorter ones so that recovery time is made more efficient. The necesity of switching to shorter esters toward the end of a cycle depends on the type of drugs used. Longer esters such as deca and eq should be replaced with shorter acting versions of these compounds no later than four weeks before the end of a cycle. Medium length esters such as t-enanthate and cypionate should be replaced no later than three weeks before the end of a cycle. A couple examples of appropriate replacements are: trenbolone acetate and testosterone propionate. There is no need to "load" these compounds in the middle of a cycle since 1) they are already "fast acting" and 2) blood androgen concentrations are already high.
4) Recovery With the replacement of the faster acting injectables toward the end of a cycle, the "wasted" time between the end of a cycle and beginning of clomid therapy is reduced. For instance, if 100mg TA is used ED, clomid therapy may begin in as little as 5 days after the last shot. This tremendously impoves time efficiency. Clomid therapy usually last for four weeks. An excellent thread posted by The Iron Game describes this in further detail Clomid FAQ's .
When the above recomendations are made, your cycle itself is made much more efficient and if recovery time is made more efficient as well, time "off" AAS may very well be reduced so that the overall efficiency of AAS use over time is tremendously improved.
Andy
If you use a long ester such as deca at xmg/week, it will take you 4-5 weeks to build up to max blood concentrations possible for xmg/week. So half of your cycle is not wasted, but you are not maximizing efficiency.
When coming off a cycle, the waiting period before clomid therapy begins will vary depending on the type and dose of the AAS. If you ran 500mg/week of deca for 10 weeks, a month after your last shot, you will still have around 200mg of esterified deca in your system. This is more than enough to prevent recovery. This is the reason why recovery is more difficult with a deca (or another long acting ester).
Let's calculate the amount accumulated in the body after 6 weeks of 500mg/deca. Let's say you inject it once a week and we'll give it a 1.5 week half life. Note that injection frequency makes a huge difference in blood concentration stability but no difference in amount of esterified in the system
E (greek letter "sigma") 500*e^(ln(1/2)n/1.5) from n=0 to n=6. So after 6 weeks, about 1300mg of esterified nandrolone remain in the body.
Now lets see how long, after the initial injection, it takes to reduce to a small enough amount that permits recovery.
1300*e^(ln(1/2)n/1.5) After 3 weeks, 325 mg of esterified remain
after 6 weeks, 81 mg of esterified remain.
After 8 weeks, 32mg of esterified remain.
Most guys go with "time on=time off." This will not work with long esters as I have demonstrated above. For at least a month after your last shot you are in what I call a "time in-effiency" period where you are no longer reaping the benefits of you AAS but you are not recovering either. The goal of the modern cycle is to minimize this wasted time.
The key components are:
1) Front end loading this cuts down on wasted time in the beginning of your cycle waiting for the doses to reach full theraputic levels. This concept has been used before but (as far as I know) I was the first one to quantify it mathmatically. Zyg has taken the math one step further with a graph showing, visually, the importance. Graph of eq loading
The use of orals in the beginning of a cycle is a popular component of a cycle. While I don't feel it is a nessecity, it too is a (different) type of front end load. For the advnaced BBer, dbol should be taken in the beginning of a cycle as well as loading the injectables since the anabolic response from dbol is alleged to be by a different mechanism than most injectables. If one had to chose between a dbol load and and injectable load, in most cases, the injectable load should be prefered over the dbol load.
2) Injection frequency This is crucial to obtaining even blood concentrations of androgens. Ideally, the more often injected, the better. An acceptable rule of thumb is "inject at half of the half life." For instance, if the half life of a steroid is 7 days, this should be injected at least twice weekly. For cycles that involve multiple injectables, the injections should be fractioned out and divided up based on the injectable with the shortest half life. For instance, if you were doing a test propionate and deca cycle, the old school way to do it would be to inject the prop EOD and the deca once a week. Both compounds should not be viewed as separate, but together with total androgen concentration taken into consideration. If you injected the deca only once a week, probably along with one of the propionate injections, that day will have a much larger spike on total blood androgen concentrations. Instead, the deca should be split up and taken with the propionate injections, EOD. This way there is no one day of the week that has a "spike" and even blood concentrations are maintained throughout the week.
3) Ending the cycle Switching to shorter esters toward the end of a cycle makes perfect sence however not too many guys incorporate this practice- perhaps because of the lack of variety of drugs. The modern cycle should include replacing long ester injectables with shorter ones so that recovery time is made more efficient. The necesity of switching to shorter esters toward the end of a cycle depends on the type of drugs used. Longer esters such as deca and eq should be replaced with shorter acting versions of these compounds no later than four weeks before the end of a cycle. Medium length esters such as t-enanthate and cypionate should be replaced no later than three weeks before the end of a cycle. A couple examples of appropriate replacements are: trenbolone acetate and testosterone propionate. There is no need to "load" these compounds in the middle of a cycle since 1) they are already "fast acting" and 2) blood androgen concentrations are already high.
4) Recovery With the replacement of the faster acting injectables toward the end of a cycle, the "wasted" time between the end of a cycle and beginning of clomid therapy is reduced. For instance, if 100mg TA is used ED, clomid therapy may begin in as little as 5 days after the last shot. This tremendously impoves time efficiency. Clomid therapy usually last for four weeks. An excellent thread posted by The Iron Game describes this in further detail Clomid FAQ's .
When the above recomendations are made, your cycle itself is made much more efficient and if recovery time is made more efficient as well, time "off" AAS may very well be reduced so that the overall efficiency of AAS use over time is tremendously improved.
Andy
Last edited:

 ..hehe, i couldnt resist.
..hehe, i couldnt resist.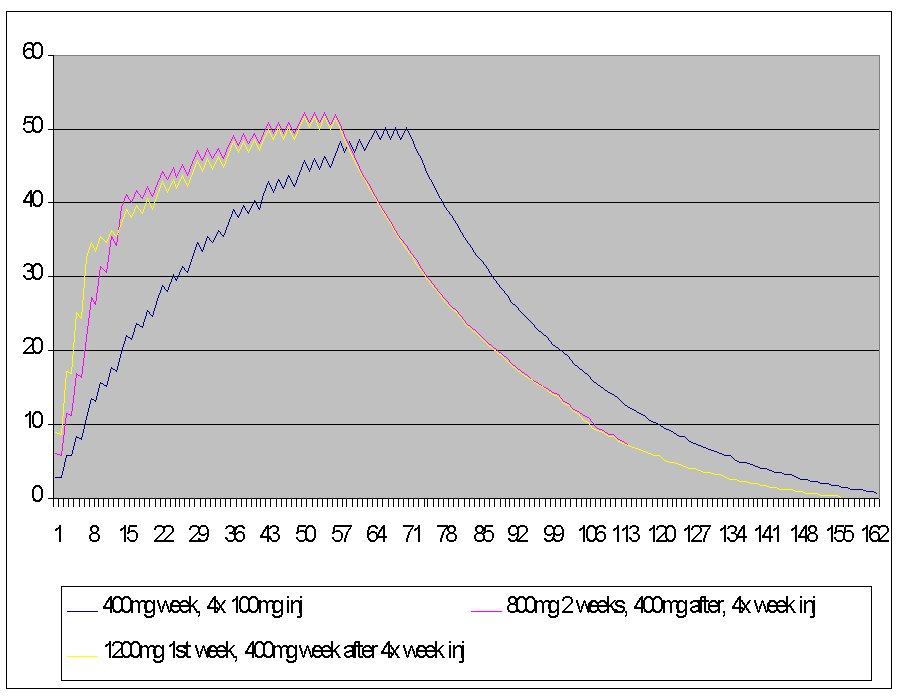

 ok I'm being funny now), and dropping out the Longer Esters.
ok I'm being funny now), and dropping out the Longer Esters.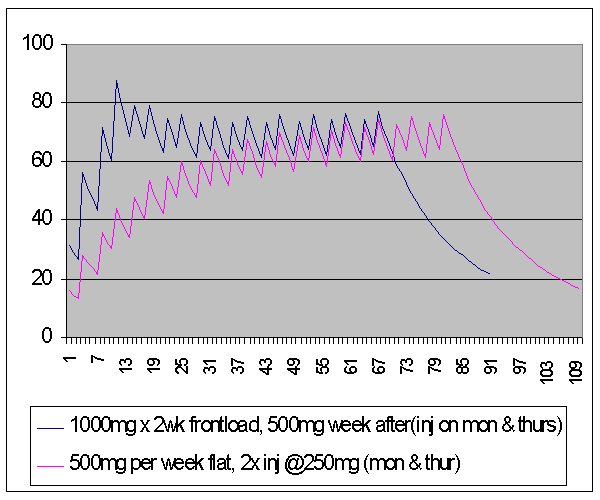
")