
















My name is Dmitry . I am 31 years old . Weight 86kg, height 1.83.
I have been training since the age of 16, for the last 2-3 years I have often been without training, but for the last 5 months I have been intensive training 3 times a week for 1:30 an hour.
Meals for the first cycle:
Protein - 297 grams (3.5 per kilogram of weight)
Carbohydrates - 301 grams (3.5 per kilogram of weight)
Fat -86 grams (1 gram per kilogram of body weight)
At 30 there was a course of 12 weeks.
1-7 weeks: turinabol 40 mg per day.
1-12 weeks: testosterone propionate.
2-12 weeks: arimidex 0.5mg every 3rd day.
Sports supplements on the course:
1) Bcaa - 10 grams per day.
2) Glutamine - 10 grams per day.
3) citrulline malate - 10 grams per day.
4) vitamins complex - every day.
5) vitamin d3: 8000 every day.
6) omega 3 - 3 grams in the morning / 1 gram in the evening.
7) vitamin E: 300 per day.
8) ZMA : 1 capsule per day.
9) Fast protein 100gr daily.
10) casein before go sleep ; 50 gr .
After the Cycle , I added tribulus 4000mg. Clomiphene citrate 50 mg per day for 3 weeks.
PCT: 6-8 weeks, depending on health and tests
Plan for the next course:
1-16 weeks : testosterone e 300 mg Monday / Friday
1-16 weeks : Primobolan 150 could Monday / Friday
2-16 weeks: anastrozole according to analyzes - 0.5-1 mg every 3 days.
16-24 weeks: testosterone cypionate 200 mg / every 8 or 10 days, I will pass the tests and understand.
The complex of sports nutrition is the same as in the first year.
Nutrition in the second Cycle :
Proteins: 275 grams (3.2 per kilogram of body weight)
Carbohydrates: 361 grams (4.2 per kilogram of body weight)
Fats: 86-100 grams per day.
Blood tests / hormones / lipid profile observed before the Cycle , during the Cycle , after.
Before the new Cycle , I will also hand over a complete list of analyzes and will continue to observe on the Cycle .
In terms of nutrition, I will add heavy carbohydrates in the morning until 16 hours. I eat every 2-3 hours.
Tes before new cycle .
Complete blood count (clinical blood count, leucocyte formula, EGAS
Iron
Transferrin
FerritinNVD
Prothrombin time
FibrinogenNVD
D-DimersNVD
Thrombin time
Bilirubin
ALAT
ASAT
GGT
LDH
CFK-Creatine kinase
Urea
Creatinine
Total protein
Albumin
Homocysteine
CRO
Sodium
Potassium
Calcium
Phosphorus
Chlorine
Magnesium
Lipid kit (HOL, LDL, HDL, TRIGL)
Prolactin
FSH
LH-Luteinising hormone
Estradiol
Progesterone
SHBG-Sex Hormone Binding Globulin
Testosterone
TSH-Thyleotropic hormone
Free T3
Free T4
Free PSA
Inhibin B.
I have been training since the age of 16, for the last 2-3 years I have often been without training, but for the last 5 months I have been intensive training 3 times a week for 1:30 an hour.
Meals for the first cycle:
Protein - 297 grams (3.5 per kilogram of weight)
Carbohydrates - 301 grams (3.5 per kilogram of weight)
Fat -86 grams (1 gram per kilogram of body weight)
At 30 there was a course of 12 weeks.
1-7 weeks: turinabol 40 mg per day.
1-12 weeks: testosterone propionate.
2-12 weeks: arimidex 0.5mg every 3rd day.
Sports supplements on the course:
1) Bcaa - 10 grams per day.
2) Glutamine - 10 grams per day.
3) citrulline malate - 10 grams per day.
4) vitamins complex - every day.
5) vitamin d3: 8000 every day.
6) omega 3 - 3 grams in the morning / 1 gram in the evening.
7) vitamin E: 300 per day.
8) ZMA : 1 capsule per day.
9) Fast protein 100gr daily.
10) casein before go sleep ; 50 gr .
After the Cycle , I added tribulus 4000mg. Clomiphene citrate 50 mg per day for 3 weeks.
PCT: 6-8 weeks, depending on health and tests
Plan for the next course:
1-16 weeks : testosterone e 300 mg Monday / Friday
1-16 weeks : Primobolan 150 could Monday / Friday
2-16 weeks: anastrozole according to analyzes - 0.5-1 mg every 3 days.
16-24 weeks: testosterone cypionate 200 mg / every 8 or 10 days, I will pass the tests and understand.
The complex of sports nutrition is the same as in the first year.
Nutrition in the second Cycle :
Proteins: 275 grams (3.2 per kilogram of body weight)
Carbohydrates: 361 grams (4.2 per kilogram of body weight)
Fats: 86-100 grams per day.
Blood tests / hormones / lipid profile observed before the Cycle , during the Cycle , after.
Before the new Cycle , I will also hand over a complete list of analyzes and will continue to observe on the Cycle .
In terms of nutrition, I will add heavy carbohydrates in the morning until 16 hours. I eat every 2-3 hours.
Tes before new cycle .
Complete blood count (clinical blood count, leucocyte formula, EGAS
Iron
Transferrin
FerritinNVD
Prothrombin time
FibrinogenNVD
D-DimersNVD
Thrombin time
Bilirubin
ALAT
ASAT
GGT
LDH
CFK-Creatine kinase
Urea
Creatinine
Total protein
Albumin
Homocysteine
CRO
Sodium
Potassium
Calcium
Phosphorus
Chlorine
Magnesium
Lipid kit (HOL, LDL, HDL, TRIGL)
Prolactin
FSH
LH-Luteinising hormone
Estradiol
Progesterone
SHBG-Sex Hormone Binding Globulin
Testosterone
TSH-Thyleotropic hormone
Free T3
Free T4
Free PSA
Inhibin B.






 It is worth noting that the thyroid activity of hCG is minimal and the drug cannot be considered a weight loss aid.
It is worth noting that the thyroid activity of hCG is minimal and the drug cannot be considered a weight loss aid. Injections can be given either intramuscularly or subcutaneously (higher bioavailability).
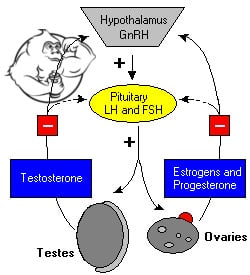
Injections can be given either intramuscularly or subcutaneously (higher bioavailability). hCG is used by men to combat azoospermia and oligospermia as a means to improve spermatogenesis, there may be variants of application against the background of primary hypogonadism (in case of violation of the hypothalamic-pituitary axis of regulation of sex hormone secretion).
hCG is used by men to combat azoospermia and oligospermia as a means to improve spermatogenesis, there may be variants of application against the background of primary hypogonadism (in case of violation of the hypothalamic-pituitary axis of regulation of sex hormone secretion).